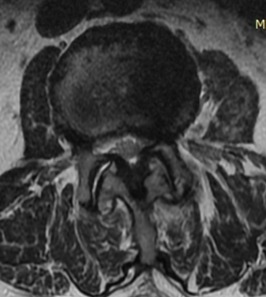
Image: Axial T2 weighted image demonstrating bilateral facet joint arthropathy with resultant mild spinal stenosis (narrowing of the central canal).
Traditionally, lumbar pain has been attributed to lumbar disc herniation or degenerative disc disease. However, there are other anatomical structures that may cause low back pain, including the facet joints, the sacroiliac joints, spinal nerve roots, muscles and ligaments, and other non-spinal causes. In the thoracic spine, each vertebra attaches to a rib on either side. Because of the inherent stability of the rib cage, symptomatic facet joint pain is less common in the thoracic spine compared with the lumbar and cervical regions. Facet joint related mid back pain usually follows surgery or trauma to that spinal segment. In the cervical spine, the facet joints are actually the most common source of pain. Neck pain is attributed to facet joint dysfunction more often than a disc herniation or to a dysfunctional intervertebral disc, combined!
Anatomy
The correct term for the facet joints is the zygapophysial joints. Typically, the zygapophysial joints are referred to as facet joints or z-joints to avoid difficult medical terminology. Each spinal segment has a pair of facet joints. The main role of these joints is to guide the motion of the spine.
Each facet joint is innervated by two nerves (most often the “medial branch of the primary dorsal rami” from two spinal levels). These sensory nerves, which transmit the signal of pain from our facet joints to our spinal cord, plays a vital role in both the diagnosis and treatment of neck and back pain from the facet joints.
Video: About Facet Syndrome
Click below to view a video from our library about this condition.
Signs and Symptoms
Lumbar spine. Low back pain originating from the lumbar facet joints can present in many ways. There exists significant overlap between pain from the facets joints and that of other spinal and non-spinal structures. (e.g. intervertebral discs, spinal nerves, sacroiliac joints, spondylolysis, etc.) Your physician may develop a high suspicion of facet joint pain after listening to your history and performing a proper physical examination; however, research has shown that it is impossible to reliably make a diagnosis without further diagnostic testing.
Thoracic spine. Mid back pain that is derived from the thoracic facet joints is quite rare. When it does occur it often presents with pinpoint pain along the spine. Sometimes it causes pain along the shoulder blade. Movements such as sideways bending, sideways rotation, or even overhead lifting may exacerbate the patient’s symptoms.
Cervical spine. Neck pain that is derived from the cervical facet joints is actually very common! Research studies show that the cervical facet joints may actually be the most common source of neck pain. However, similar to the lumbar spine, there exists significant overlap between pain from the facets joints and that of other spinal and non-spinal structures (e.g. intervertebral discs, spinal nerves, upper back muscles, muscles, TMJ, etc.). Your physician may develop a high suspicion of facet joint pain after listening to your history and performing a physical exam. Again, it is impossible to reliably make a diagnosis without further diagnostic testing.
Imaging Studies
One must recognize that imaging studies only provide anatomic detail and cannot independently determine the particular source or cause of pain. There are no radiographic studies available at present to conclusively diagnose facet joint pain. Various studies may reveal anatomic abnormalities of the spine. However, they are not diagnostic. Due to the fact that pain is a subjective experience, the spine physician must carefully assess the history and correlate it with the imaging studies. Use of plain radiographs, CT, CT myelography, MRI, bone scans and SPECT can be utilized to provide additional anatomic detail. They can also alert the physician of malignant causes of spine pain.
Diagnostic Injection
Spine physicians may use intra-articular (joint injection) or medial branch blocks (nerve blocks) for the diagnostic work up. If your physician suspects that your back or neck pain is emanating from the facet joints, they must perform a diagnostic injection series to confirm this suspicion. Under live x-ray guidance, local anesthetic is precisely injected to block the nerves that give sensation to the joint in question (medial branch block). If this provides complete or near complete relief of your neck pain, it is likely that the joint is the culprit. However, if you obtain good relief, the block must be repeated a few days later, with a different medication. This is done to make sure your response to the original block was not a false-positive result (“placebo effect”). Believe it or not the rate of false-positives is greater than 30%!
Treatment
Various treatment options are available for facet joint pain.
Radiofrequency neurotomy. The standard of care is a radiofrequency neurotomy or radiofrequency ablation. Facet neurotomy is a procedure procedure that interrupts the pain signal through a facet joint’s nerve. A radio-frequency probe that heats the 2 small nerve branches to each facet joint accomplishes this interruption known as denervation.
Intra-articular steroid injection. There are a definite percentage of patients who suffer from joint pain that will respond the instillation of corticosteroids into the affected joint(s). This is a quick, safe procedure that is easy to tolerate. However it is typically only recommended in select patients because the results from this procedure do not measure up to those of radiofrequency neurotomy.
Intraarticular Platelet-Rich Plasma (PRP) injection
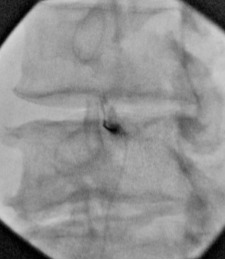
Image: Oblique view of the left L3-4 facet joint. This is a fluoroscopic image of the spinal needle placed in the posterior left L3-4 facet joint. 1 can see a small amount of radiopaque contrast tracking upward toward the top of the joint.
There is growing evidence and consensus support for the treatment of facet joint pain with intraarticular and periarticular PRP injections. While radiofrequency ablation (radiofrequency neurotomy) remains the standard of care (best studied and most accepted treatment for facet joint pain), there is a growing role for orthobiologics (The products used in regenerative medicine) in the treatment of facet joint pain: 1) The most obvious scenario is the younger patient who has a leading diagnosis of facet joint pain but does not want to commit to radiofrequency neurotomy as their treatment of choice every one or two years for the foreseeable future (I.e. repeated ablations). Trying an alternative treatment that might offer long-term results without the need to undergo ablation of tissue is enticing in this patient cohort. 2) Other patients may express fear or apprehension for undergoing radiofrequency neurotomy, despite the low risk of complications. 3) Other patients have a preference for procedures that are theoretically “regenerative” rather than those that are, technically, “destructive” (E.g. radiofrequency ablation).
Physical therapy
- Education and training in proper body mechanics and posture are essential.
- Strength training. A sound foundation for your spine to work from will help with long-term results. Gaining stability in your pelvic and shoulder girdles will set you up for sustained benefit from your facet neurotomy.