Sciatica
Most patients have heard the phrase “sciatica”. The term sciatica is used for descriptive purposes only. What most patients are unaware of is that the sciatic nerve is the least likely anatomical structure involved in causing their low back and leg pain. The term radiculopathy (dysfunctional nerve root) is much more accurate. Radiculopathy refers to compression or irritation of a spinal nerve, as it leaves your spinal canal, resulting in low back pain radiating into the buttock and/or leg.

Video: About Sciatica
Click below to view a video from our library about this condition.
The main causes of radiculopathy include:
- Lumbar Disc Herniation. A disc herniation is the most common cause of sciatica. You may be familiar with the terms protrusion, extrusion, sequestration, or bulging. A qualified spine physician may explain how of each of these descriptive terms may be relevant to your problem.
- Spinal Stenosis. The term stenosis simply means, “narrowing”. There are three main types of stenosis
- Central canal stenosis

- Foraminal stenosi
- Lateral recess stenosis.
The fancy medical naming of each type of stenosis is unimportant for this basic discussion. In general,stenosis usually refers to arthritic that your spinal nerve(s) must pass through and exit to leave your spinal column and travel to your leg.
The narrowing can actually be secondary to a combination of factors
- Arthritic narrowing
- Lumbar Disc herniation
- Spondylolisthesis
- Compression from a degenerative cyst
Most cases of sciatica do not require surgery. Whether your sciatica symptoms are caused by a disc herniation or spinal stenosis, you have a good chance of recovery with non-surgical treatment. Surgery is reserved only for the most serious cases or those resistant to non-surgical care.
Symptoms
Symptoms of a lumbar disc herniation may include the following:
- Dull or sharp pain in the lower back, intensified by movements or activities such as bending, coughing, or sneezing.
- Muscle spasms or cramping.
- Sciatica (pain, burning, tingling, and numbness that extends from the buttock into the thigh, leg or foot).
- Leg weakness or loss of leg function.
Diagnosis
Good treatment is always based on an accurate diagnosis. A comprehensive diagnostic process includes:
- Medical history. Your physician will talk to you about your symptoms, how severe they are, and what treatments you have already tried.
- Physical examination. You will be carefully examined for limitations of movement, problems with balance, and pain. During this exam, your physician will also look for loss of reflexes in the extremities, muscle weakness, loss of sensation or other signs of spinal cord damage.
- Diagnostic tests.
- MRI. MRI provides the most accurate three-dimensional views of the lumbar spine and can help detect herniated discs. It can also help rule out other disorders of the spine that may mimic the symptoms of a disc herniation.
- EMG. EMG is an electrodiagnostic study (nerve test) that may help clarify definite injury to one particular nerve root. This test may also give the physician feedback as to the severity of this nerve injury.
- Diagnostic Selective Nerve Root Block. A diagnostic selective nerve root block (SNRB) is similar to other spinal injections that a patient may undergo. However, this injection is purely diagnostic in nature (not a treatment), aiding you physician in confirming your suspected diagnosis.

Sagittal T2 weighted image of the lumbar spine. A moderate sized L5-S1 disc protrusion is displayed.
Sagittal T2 weighted image of the lumbar spine. A moderate sized L5-S1 disc protrusion is displayed.

Sagittal T2 weighted image of the lumbar spine. A moderate sized L5-S1 disc protrusion is displayed.
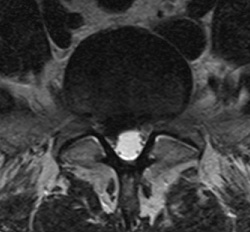
Axial T2 weighted image of the lumbar spine. The same L5-S1 disc extrusion, is displacing and compressing descending left S1 nerve root.

Sagittal T2 weighted image of the lumbar spine. Small to medium sized disc protrusion at L4-5.
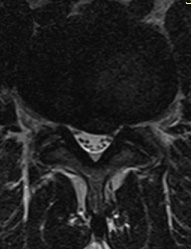
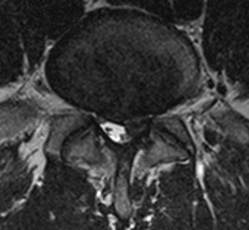
Axial T2 weighted image of the lumbar spine. The same L4-5 disc protrusion is potentially compromising the descending left L5 nerve root.
Treatment for Sciatica
Most cases of sciatica do not require surgery. Whether your sciatica symptoms are caused by a disc herniation, foraminal stenosis, or lateral recess stenosis, you have a good chance of recovery with non-surgical treatment. Surgery is reserved only for the most serious cases or those resistant to non-surgical care.
Non-Operative Treatment
A combination of the following treatments will be used with most sciatica patients:
- Medications
- Anti-inflammatories: to reduce swelling and pain
- Narcotic painkillers: to alleviate acute pain (only if absolutely necessary)
- Physical therapy. An exercise prescription tailored to your condition will be prescribed to direct your physical therapist. A typical prescription involves:
- Stretching exercises
- Strengthening exercises
- Core stability training
- Balance training
- A therapeutic selective nerve root block (SNRB) series. This is otherwise known as a transforaminal epidural steroid injection (TFESI).
- Most patient s will benefit form a type of pinpoint epidural injection, under live x-ray guidance, of a strong anti-inflammatory medication (corticosteroid)
- Maximum benefit typically occurs following 1 to 3 injections
Surgical Treatment
If you are not improving, then you may be recommended for surgery to relieve the irritation or compression of the injured nerve.
Surgical Indications:
- Intolerable pain despite medical management
- Evidence of progressive (worsening) neurological deficit (e.g. significant weakness and/or numbness)
- Bowel or bladder dysfunction
- Failure to improve following a reasonable course of interventional/medical management