Cervical Facet Radiofrequency Neurotomy “Radiofrequency Ablation” (RFA)
If you have been diagnosed with cervical facet joint pain (zygapophysial joint arthropathy) you may be a candidate for a cervical radiofrequency neurotomy. Neurotomy is a procedure which results in interruption of the nerve supply to a facet joint. This interruption, known as denervation, is accomplished by a radio-frequency (RF) probe that heats the 2 small nerve branches to each facet joint. From the C3-4 through C7-T1 levels in the cervical spine (neck) these nerves are called the medial branches. At the C2-3 level, the nerve is called the third occipital nerve (TON).
Video: Cervical Facet Radiofrequency Neurotomy
Click below to view a video from our library about this procedure.
How is it Done?
The procedure is performed in an operating room or procedure suite. With the patient in a prone position (on your stomach) and under local anesthesia (skin is frozen with numbing medication) and fluoroscopic (live x-ray) guidance, a radio-frequency needle is advanced to the base of the spinal bone that the nerve runs along. The needle is placed along the course of the appropriate nerve (medial branch of the dorsal ramus). The needle is heated to 80 degrees C for 90 seconds. At least 2 branches for each joint are treated in this same manner. Each branch may be heated 2-4 times to achieve a full clinical effect.


Image: Lateral images from different patients. The image on the right displays a radiofrequency needle placed at the C3 bony level, targeting the right C3 medial branch nerve. The image on the left demonstrates a radiofrequency needle placed at the C6 bony level, targeting the C6 medial branch nerve.
How Long Does it Take?
The neurotomy takes between 45 minutes and an hour and a half, depending on the number of levels to be done. The patient is then brought to the recovery area for 30 minutes of observation.
Potential Risk
The risks of this procedure are small. Theoretically, there is a risk of nerve damage to the larger spinal nerve where medial branch of the dorsal ramus originates. However, 3-step safety precautions are taken to avoid this and true nerve damage is quite rare.
At the C2-3 level, you may experience a patch of numbness at the base of your skull after the procedure. This is expected after a neurotomy of the third occipital nerve (TON).
At the C3-4 level, you may experience a patch of numbness at the bottom of your neck after the procedure. This may occur after a neurotomy of the deep branch of the medial branch nerve at C3.
It is not uncommon to experience increased localized burning, itchy neck pain for 1-2 weeks from the time of the procedure. Rarely these irritating symptoms may persist for weeks or months following the procedure. You should discuss this risk with your doctor.
As with any injection procedure, there is a remote risk of bleeding or infection.
Expected Outcome
Following the neurotomy, there is a 60 to 70% chance of complete or near complete pain relief. This typically lasts for 9 to 11 months. However, the duration of relief can range from 6 months to 3 years. The nerve eventually grows back and the procedure can be repeated.
Lumbar Facet Radiofrequency Neurotomy “Radiofrequency Ablation” (RFA)
If you have been diagnosed with lumbar facet joint pain (zygapophysial joint arthropathy) you may be a candidate for a lumbar radiofrequency neurotomy. Neurotomy is a procedure which results in interruption of the nerve supply to a facet joint. This interruption, known as denervation, is accomplished by a radio-frequency (RF) probe that heats the 2 small nerve branches to each facet joint. These nerves are called the medial branches.
Video: Lumbar Radiofrequency Neurotomy
Click below to view a video from our library about this procedure.
How is it Done?
The procedure is performed in an operating room or procedure suite. With the patient in a prone position (on your stomach) and under local anesthesia (skin is frozen with numbing medication) and fluoroscopic (live x-ray) guidance, a radio-frequency needle is advanced to the base of the spinal bone that the nerve runs along. The needle is placed along the course of the appropriate nerve (medial branch of the dorsal ramus). The needle is heated to 80 degrees C for 90 seconds. At least 2 branches for each joint are treated in this same manner.

Image: Right L3 medial branch ablation located at the L4 bony level.
How Long Does it Take?
The neurotomy takes between 45 minutes and an hour and a half, depending on the number of levels to be done. The patient is then brought to the recovery area for 30 minutes of observation.
Potential Risk
The risks of this procedure are minimal. Theoretically, there is a risk of nerve damage to the larger spinal nerve where medial branch originates. However, 3-step safety precautions are taken to avoid this and true nerve damage is almost unheard of.
It is not uncommon to experience increased localized neck pain for 1-2 weeks from the time of the procedure.
As with any injection procedure, there is a remote risk of bleeding or infection.
Expected Outcome
Following the neurotomy, there is a 70% chance of complete or near complete pain relief (depending on the degree of relief from your diagnostic medial branch blocks!) This typically lasts for 10 months to 12 months. However, the duration of relief can range from 6 months to 3 years. The nerve eventually grows back and the procedure can be repeated.
Thoracic Facet Radiofrequency Neurotomy
The most common scenario for the development of thoracic spine facet joint pain is trauma. Perhaps the most common of all scenarios is the experience of a vertebral body compression fracture, either through trauma or through an osteoporotic insufficiency fracture. This can disturb the alignment of the local anatomy. This can put stress on the posteriorly located anatomy, such as the thoracic facet joints. If you are diagnosed with thoracic spine facet joint pain, you may be a candidate for radiofrequency ablation of the small nerve endings that feed the thoracic facet joints. Similar to the cervical spine above and the lumbar spine below, these nerves are termed the medial branch nerves. Radiofrequency ablation is a relatively simple procedure with a moderate success rate for long-term relief of thoracic facet joint pain.

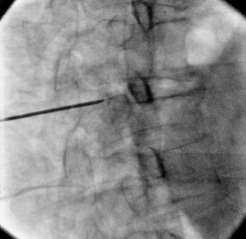
Image: AP and oblique images of a thoracic radiofrequency ablation targeting the right T7 medial branch nerve. The oblique image on the right side shows evidence of a moderate compression fracture of the T7 vertebral body.
The RFA procedure is not targeting the innervation of the fracture. Rather, the RFA procedure is targeting the medial branch nerves which innervate the facet joints immediately posterior to (behind) the fracture.